As a contracted wound ostomy continence nurse across a rural 100-mile radius in Northeast Nebraska for the past 16 years, I have witnessed that rural wound care is largely dictated by reimbursement. Comprehensive reimbursement is best achieved when performed in the outpatient clinic. However, outpatient clinic reimbursement is only as effective as the documentation and coding of the rural hospital to which it is attached, and effective chargemasters are a contract nurse’s best friend.
Throughout the course of patient care, every encounter is documented and becomes part of the legal medical record. This medical record serves to plan and provide continuity of care for medical treatment.1 However, in a series of practice points, Hess states, “Healthcare providers need to also remember the additional functions of the medical record, including the following: providing information for the financial reimbursement to hospitals, healthcare providers and other sites of service, and patients.”1
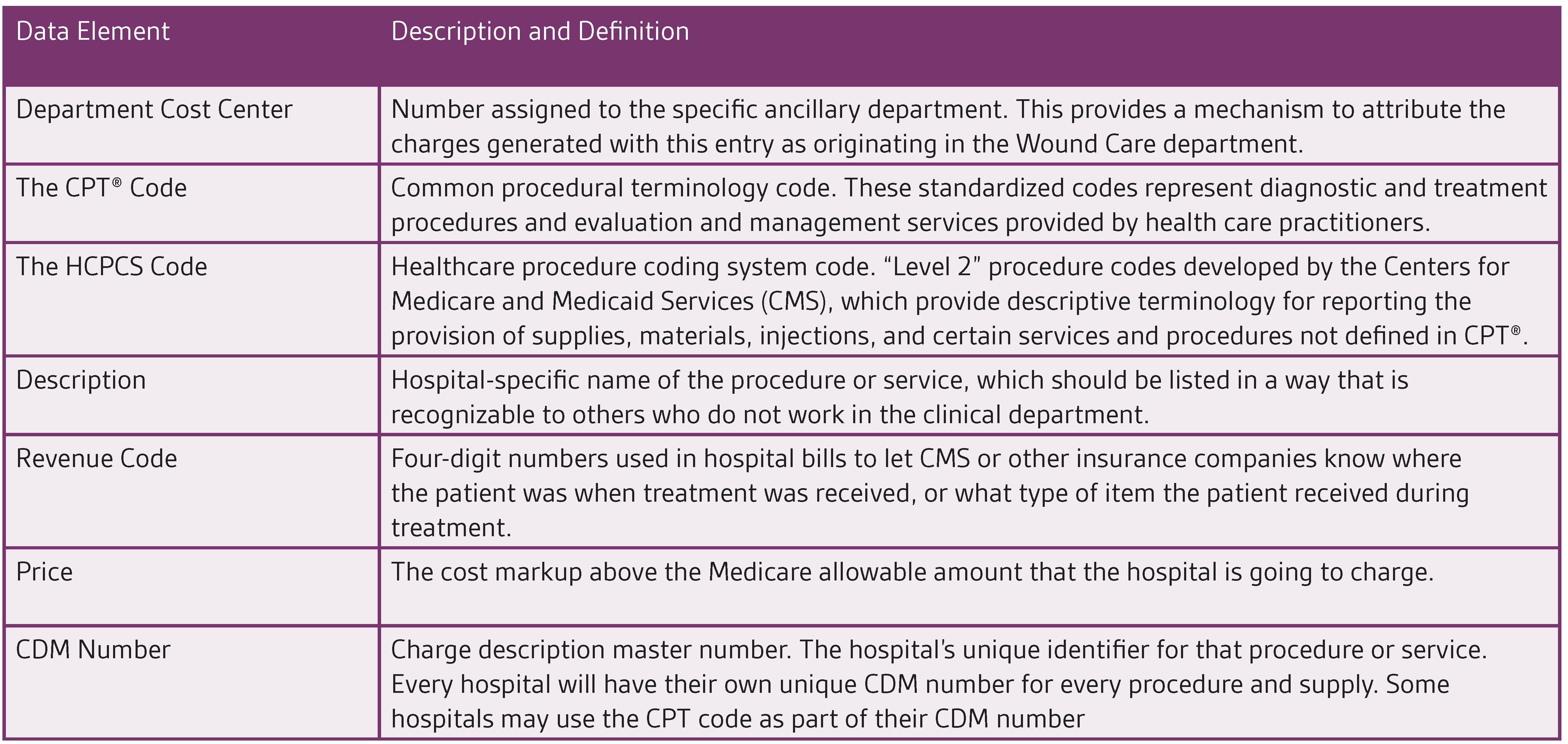
In a 2007 article from Today’s Wound Clinic, it was noted that “before the patient can be seen, the clinic has to determine how it will prepare a bill (charges) for the services rendered to the patient.”2 This means that each hospital clinic should develop a chargemaster specific to their department to capture charges and ensure consistent billing. While the layout of individual facility chargemasters varies from facility to facility, it includes a core group of data elements corresponding to all of the services, procedures, and supplies that may be used.2 The description of these key corresponding data elements is outlined in Table 1:2
In my experience, documentation for wound care services has varied and often the information needed to obtain full reimbursement was not being asked. Therefore, the coding of services, procedures, and tests was destined to be inaccurate and incomplete causing major shortcomings in the ability of the outpatient facility to capture full reimbursement for the procedure or service in question. With many hospital and facility administrators looking at the finer details of their contract agreement instead of internal inefficiencies which impacted the facility’s reimbursement, the conclusion was that this reimbursement gap was being driven by contractor pricing.
To remedy these shortcomings in documentation and to provide a strong foundation from which outpatient clinics could develop accurate billing practices, nurses may choose to rely on application writers. In addition, there are several web-based applications available on the market that offer advanced wound and ostomy documentation with the ability to add individual treatments and perform detailed assessments. Many of these applications are able to deliver true point of care service by bringing convenient and immediate wound care to the patient. Thus, my time with documentation is minimized and the facility I am contracted to has the procedures I have performed automatically sorted in an easy to decipher coding-ready report.
Typically, hospital billing administrators may not have full confidence in the contractor in regard to knowledge of their chargemasters. To remedy this problem, enlisting the help of both suppliers and coders can be beneficial, since suppliers know how well their product and the procedures associated with their product can be most effectively reimbursed.
Gaining the trust of the facility’s coder and building a strong working relationship is a critical piece of the overall puzzle of ensuring accurate documentation and maximal reimbursement for facilities. Working with coders who are well-informed in the use of the local coverage determination in wound care is the best way to ensure that information about procedures and services is captured and documented accurately to maximize reimbursement.
Another important aspect of wound care in an outpatient setting involves the ability for the practitioner to deliver patient-centric care on an individualized basis by combining an evidence-based approach with the ‘art’ of wound healing. For example, diabetic foot care is a chronic problem in wound care that can leave the clinician continuously searching for new treatment strategies. Because of the high rate of diabetic foot ulcers resulting in amputation, it is important to work with facilities that have a defined treatment protocol and approach to wound management, so that individual knowledge can be applied to generate optimal outcomes for patients.
Keeping oneself free from facility policy that may impinge upon practice management is not always easy to do as some wound, ostomy, continence nurses in large facilities have found. Limitations on product utilization may result in treatment stagnation as a result of policies drawn up by people in a large, complex system where pre-existing silos between finance and clinical departments can often conflict.
In the larger settings of urban outpatient clinics, there is room at the top of the organizational structure for the practicing wound, ostomy, and continence nurse to migrate from the day-to-day management of patients to duties of a more administrative nature. With this in mind, it is important for nurses to remember that no matter the setting, adhering to strong practice principles along with a fastidious commitment to documentation and proper coding of services and procedures, overall patient outcomes and facility reimbursement can both intersect to achieve important milestones.
© 2021 3M. All right reserved. 3M and the other marks shown are marks and/or registered marks. Unauthorized use prohibited. 3M marks used under license in Canada. All other marks are property of their respective owners. [PRA-PM-US-03289 (07/21)]